biologics for Rheumatologists, how do they defer from chemical drugs
IF you are diagnosed with autoimmune disease, not necessarily Rheumatological, you might have heard the word biologics and got confused – rightly so. I will mainly talk about biologics for Rheumatologists. To simplify, most traditional medications are extracted from plants, animals, and all sort of living creature and purified. They usually have basic chemical structure that you can write such as methotrexate “C20H22N8O5”.
Traditional medications are made from basic elements like carbon, hydrogen, nitrogen, and oxygen. Basically, drugs are made through chemical reactions in tubes. They are so basic that they interact with several areas in our human body. I heard a pharmacist call them pharmaceutically promiscuous. Meaning they bind and work on several areas. Which makes them work for a lot of issues and diseases. They are not that strong unless you use huge doses which would start causing intolerable side effects.
Initial discovery of biologics
Later, science evolved to find certain proteins that work too much in autoimmune disease. So, the idea came of using a medication, that goes to that protein and stops it from working, will make the disease less active. To block proteins, you need proteins. If you look at levels of protein structure, you will realize that they are complex. Look at this website first picture https://byjus.com/chemistry/protein-structure-and-levels-of-protein/.
It is quite impossible to just make proteins from a chemical reaction, at least not with a certain shape. We therefore ask cells to make them. We use the live cell’s ability to make proteins. We sort of just give them the code for it. Which makes these medications made in biological structures -the cells.
Umbrella concepts for biologics and potential side effects
what are umbrella concepts of biologics? It was found that biologics are quite effective at what they do typically and alter the immune system. Individuals using them have higher risk of infection. Note here, I said higher risk and not “amount”. For example, 1000 people with a disease would still get infections, maybe 5 each year. If they take classical pharmacological promiscuous medications, such as methotrexate, 8-10 out of 1000 will get infections. If a biologic is used, then 10-15 out of the 1000 will get infections each year. Note also that not all are serious infections, they could be simple uncomplicated urinary tract infections.
Note also because they are effective, although controversial, it is thought that they increased risk of cancer BUT NOT ALL OF THEM. I said controversial as there is hypothesis that autoimmunity could be a mechanism to protect against a hidden cancer, so you just remove the covering OR that autoimmune disease themselves makes humans prone to cancers. On the latter point, I am not suggesting that cancer is common in autoimmune disease patients. Again, the increased risk does not necessitate any additional cancer screening than required to general population.
Autoimmune muscle disease (i.e. dermatomyositis and myositis) is the only disease that requires a bit more vigilant cancer work up due to clear increased risk of cancer. Going back to biologics, due to being proteins that your body might recognize as foreign, allergic reaction are a possibility but there are protocols to deal with reactions.
How does Rheumatologist choose what biologics for Rheumatoid arthritis or other disease?
What about the choice of biologics for Rheumatoid arthritis. In simple terms, there is no 100% agreed upon sequence. The main rule is that we look at your medical history. We choose the medication that causes the least issues for you. We choose the medications that do not cause worsening of your medical issues. We obviously try to choose the strongest medication based on our experience. Keep in mind, there is generally no clear proof that one biologic is better than another.
Rule of thumb for Rheumatoid arthritis, we try to start with anti-TNF medications such as Humira, Remicade, Enbrel, and cimzia. At times, it is easier for patients to do infusions (staying in a clinic and taking the medication through the vein directly), at other times it is easier for patients to use a pen with a needle to self-inject the medication at home. At times, insurance prefers one biologic over another due to their Rheumatologist guidelines or possibly cost benefit. So now I list the commonest biologics and their pros/cons.
Keep in mind, for all biologics we screen latent TB (carrier of tuberculosis) and viral hepatitis. If positive, then a special discussion will happen with your rheumatologist. But let us start with the list:
Anti-Tumor necrosis factor biologics for Rheumatologists
Humira an anti-TNF architype, one of the oldest biologics and is quite effective. It is self-injectable. We do not use it in people with heart failure that is related to reduction of heart pumping ability called ejection fraction (EF). If EF is low, we avoid all Anti-TNF.
Enbrel is also in the category of anti-TNF. Its way of working is slightly different though, which could lead to higher risk of autoimmune eye disease, therefore it kind of dropped to second or even completely at times. In setting for Rheumatoid arthritis though, it generally does not lose effect if given without methotrexate. Other anti-TNF typically would have higher chance of failing if given without methotrexate.
Remicade an infusion based anti-TNF. Preferred in setting of easing compliance to patient as they don’t have to depend on injecting themselves and forgetting. Also, its dose could be adjusted in contrast to most self-injectables that are standard dosing. I used it for patients when they have partial effect on injectable anti-TNF.
Cimzia is a special anti-TNF that we can use during pregnancy as the protein is large enough that it does not reach the fetus, at least not in significant amounts. With this one, you do not need to adjust your baby’s vaccine schedule.
Simponi (subcutaneous) and Simoni aria (infusion) are another anti-TNF, less likely to cause reaction compared to Remicade, probably, but its dose is generally not adjustable.
Interleukin 6 inhibitor biologics for Rheumatologists
Actemra as architype of IL-6 inhibitors. IL-6 is made at the liver. Acterma can at times affect the liver, increase triglyceride levels (type of bad fat), and lower white cell count (this one is not common). Therefore, we watch liver function, blood count, and triglyceride. Keep in mind, we do not freak out on the slightest elevation in these tests. Quick drastic changes are what make us stop medications.
Due to these possible side effects, I stay away from this med in patients with liver disease (not just fatty liver, more of fibrosis) and high risk cardiac and stroke issues patients. Kevzara is another one in this category. On rare occasions, this medication has been connected with bowel issues, so I avoid it in patients who has bowel aneurysm or history of ruptures.
Preventing B/T cell talk biologics for Rheumatologists
Orencia. Somehow, I noted that I lean to use this one when patients have problems complying with lab monitoring or had allergic reaction to anti-TNF or other meds. I avoid this medication in patients with lung issues from smoking. It seems it is a well-tolerated medication with low reaction, but this is solely based on experience.
B-Cell suppression biologics for Rheumatologists
Rituximab: This is an older drug that is part of some blood cancer therapies. Generally, well tolerated and works for multiple autoimmune disease and more notably lung inflammation from autoimmune disease -called nonspecific interstitial pneumonitis-NSIP. It has a super rare side effect which is a type of brain infection. It is rare enough that I will likely retire or die myself and I won’t see this side effect in my patients. Generally, most Rheumatologist would give this medication when we do not have other options for Rheumatoid arthritis. For example, general wisdom dictates that if a patient has history of cancer that Rituximab has the least likelihood to cause cancer as it is USED to TREAT blood cancers.
Closing remarks
I listed the most used Rheumatoid arthritis biologics. These are commonly combined with disease modifying chemical agents such as methotrexate. I hope this gives some simple explanation why your rheumatologist chooses one drug over another. Keep in mind as a relatively rare kind of docs, we each have unique experiences with these meds. Also keep in mind that these meds are getting something sort of generic called biosimilar. You might hear inflectra and it is simply a bio-similar to Remicade. Rheumatologists to a degree are being acquainted with new meds or new generics and we have varied opinions about them too.
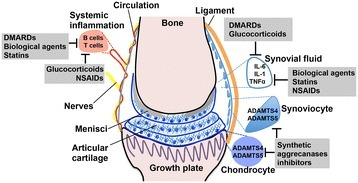
Dancevic CM, McCulloch DR -Arthritis research & therapy(2014) https://creativecommons.org/licenses/by/4.0/



Comments
Pingback: How to manage ankylosing spondylitis effective guidance 4 main categories - Medical Hermit
Pingback: Chemically Targeted Treatment for Rheumatoid arthritis quick guidance on 3 famous ones - Medical Hermit