
Introduction
How the idea of Chemically Targeted Treatment came by? At one point, all newer stronger medications for Rheumatoid arthritis were injectable through subcutaneous injection or intravenous. The reason: these were proteins, if ingested, would be destroyed by stomach acids. These are called biologics. Then I used to joke and say, “the dude/gal who will find a biologic that is a pill, would be a billionaire”. This statement was a bit short sighted. Although biologics was not switched to being pills, there came a category called small molecule targeted therapy.
So as biologics, they are designed to go and attack as specific area of the immune system. They are small enough to be absorbed into the blood stream. People who hate injections were elated and happy. Rheumatologists got somewhat excited. This category worked for Rheumatoid arthritis, psoriatic arthritis, and inflammatory bowel disease (ulcerative colitis and Crohn’s). There is even a study for possible use in ankylosing spondylitis. The results were not that awesome though for lupus.
Why less preferred by some experts?
“Doc, you have a sad tone in the paragraph above”. Yes, I do. Keep in mind that even after the federal drug administration approves a medication, it pushes for long term side effects study. It is not a choice. I mean studying things more is good to feel better. The results here are somewhat disappointing. That is why some Rheumatologist, keep these drugs as last solution. For one, they require monitoring that other biologics do not need. Secondly, there are some side effects that generally doctors frown upon. I will summarize them from the article I used below as a resource.
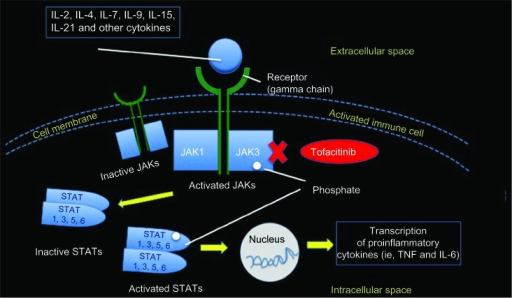
The tyrosine kinas inhibitors
There are three famous tyrosine kinase inhibitor small molecules: Xeljanz (oldest), Olumiant, and Rinvoq (coolest kid on the block). The story started with noting more heart disease (like heart attacks) and veinous clotting in Xeljanz patients. That was the first bummer. Mainly these issues were seen in older female patients. Maybe this contributed to a higher chance of issues.
Hearing that, however, will let me try avoid in such patients. Rinvoq when compared to anti-TNF (first biologic recommended after DMARDS), there was no higher risk of clots, cardiovascular disease (heart attacks and strokes), nor cancers. BUT there were higher liver issues and shingles. Rinvoq did evade the Xeljanz/Olumiant clotting and cancer issues. However, Rinvoq showed higher risk of death, hospitalization and disability in comparison to Xeljanz in united stated side effects reporting data.
Verdict
Generally, I only prescribe this category when I am continuing medication prescribed by prior Rheumatologist. I usually, however, re-counsel patients of the medications side effects. I will continue looking for future data that might support these meds. I will keep a look out for altered tyrosine kinase inhibitors that have less of these side effects.
Resources:
https://www.jmcp.org/doi/full/10.18553/jmcp.2022.28.9.1046
Cutolo M, Meroni M -Journal of inflammation research(2013) https://creativecommons.org/licenses/by-nc/3.0/


